A varicocele is an enlargement of the veins that transport oxygen-depleted blood away from the testicle. A varicocele is an enlargement of the veins within the loose bag of skin that holds your testicles (scrotum). A varicocele is similar to a varicose vein you might see in your leg.
Varicocele treatment might not be necessary. Many men with varicoceles are able to father a child without any treatment. However, if your varicocele causes pain, testicular atrophy or infertility or if you are considering assisted reproductive techniques, you might want to undergo varicocele repair.
The purpose of surgery is to seal off the affected vein to redirect the blood flow into normal veins. In cases of male infertility, treatment of a varicocele might improve or cure the infertility or improve the quality of sperm if techniques such as in vitro fertilization (IVF) are to be used.
Clear indications to repair a varicocele in adolescence include progressive testicular atrophy, pain or abnormal semen analysis results. Although treatment of a varicocele generally improves sperm characteristics, it's not clear if an untreated varicocele leads to progressive worsening of sperm quality over time.
RISKS
These are the commoner risks. There may be other unusual risks that have not been listed here. Please ask you surgeon if you have any general or specific concerns.There are risks associated with any anaesthetic.You may have side effects from any drugs used. The commoner side effects include light-headedness, nausea, skin rash and constipation.
The correction of a Varicocele has very few risks but can include:
- Build-up of fluid around the testicles (hydrocele)
- Recurrence of varicoceles
- Infection
- Damage to an artery
Some of the above risks are more likely if you smoke, are overweight, diabetic, have high blood pressure or have had previous heart disease.
Method of repair used: Open surgery.
This treatment usually is done during general anaesthetic. Commonly, your surgeon will approach the vein through your groin (inguinal or subinguinal), but it's also possible to make an incision in your abdomen or below your groin.
Advances in varicocele repair have led to a reduction of post-surgical complications. One advance is the use of the surgical microscope, which enables the surgeon to see the treatment area better during surgery.
Another is the use of Doppler ultrasound, which helps guide the procedure.
You might be able to return to normal, nonstrenuous activities after two days. As long as you're not uncomfortable, you might return to more strenuous activity, such as exercising, after two weeks.
Pain from this surgery generally is mild but might continue for several days or weeks. Your doctor might prescribe pain medication for a limited period after surgery. After that, your doctor might advise you to take over-the-counter painkillers, to relieve discomfort.
Your doctor might advise you not to have sex for a period of time. Most often, it will take several months after surgery before improvements in sperm quality can be seen with a semen analysis. This is because it takes approximately three months for new sperm to develop.
Open surgery using a microscope and subinguinal approach (microsurgical subinguinal varicocelectomy) has the highest success rates when compared with other surgical methods.
When you are discharged, take care of the following:
- Take it easy for the first 2 days after the procedure to minimise the risk of bleeding and bruising
- Wear firm-fitting underwear to help minimize bleeding
- You can remove your dressing/plaster after 2 days
- Sexual activity can be resumed after 1 week if you are comfortable
- Finish all prescribed medication
- Contact your doctor if you have severe pain, bleeding or fever

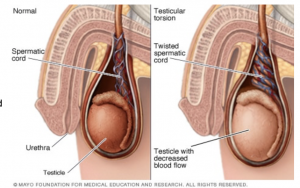 rotates on the spermatic cord, which brings blood to the testicle from the abdomen. If the testicle rotates several times, blood flow to it can be entirely blocked, causing damage more quickly.
rotates on the spermatic cord, which brings blood to the testicle from the abdomen. If the testicle rotates several times, blood flow to it can be entirely blocked, causing damage more quickly.