BRACHI THERAPY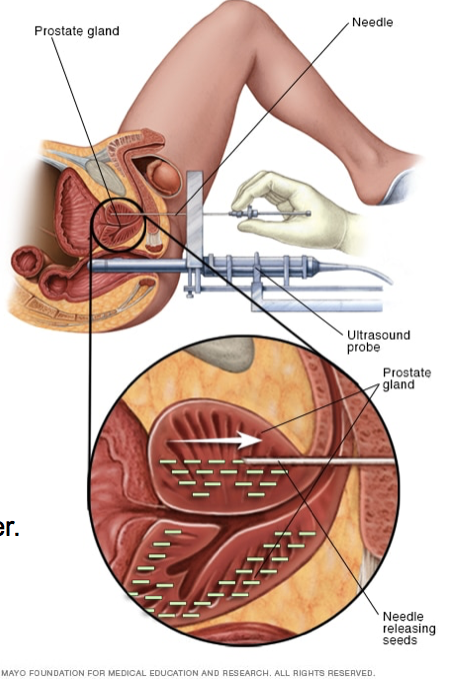
Prostate brachytherapy is a form of radiation therapy used to treat prostate cancer. Prostate brachytherapy involves placing devices containing radiation in the prostate gland close to the cancer cells.Permanent prostate brachytherapy involves placing radioactive seeds in the prostate gland permanently, where they slowly release radiation.The goal of prostate brachytherapy is to place the radiation close to the cancer cells, where the radiation can kill the cancer cells while causing less damage to healthy tissue nearby.After prostate brachytherapy, you can expect some pain and swelling in the perineum where the radiation needles were inserted. You may find relief by placing an ice pack over the area or taking acetaminophen (Tylenol, others). Tell your doctor if these measures aren't controlling your pain.You can resume normal activities when you feel up to it. Avoid strenuous activity, such as running, or activities that may irritate the perineum, such as riding a bike, until the area where the radiation was inserted is no longer tender.
RISKS
These are the commoner risks. There may be other unusual risks that have not been listed here. Please ask you surgeon if you have any general or specific concerns.There are risks associated with any anaesthetic, you may have side effects from any drugs used. The commoner side effects include light-headedness, nausea, skin rash and constipation.
Some potential adverse reactions related to Brachi Therapy include:
- Difficulty starting urination
- Frequently feeling an urgent need to urinate
- Feeling a burning sensation when urinating
- Blood in urine
- Needing to urinate at night
- Not being able to empty your bladder completely
- Narrowing of the tube that carries urine from your bladder to the outside of your body (urethra)
- Erectile dysfunction
- Bleeding from the rectum
- Blood in stool
- Diarrhoea
Some of the above risks are more likely if you smoke, are overweight, diabetic, have high blood pressure or have had previous heart disease.
When you are discharged, take care of the following:
- You can expect swelling and bruising of the scrotum and perineum (the area between the scrotum & anus) this should resolve in 1-2 weeks.
- Ice packs and over the counter medications such as Panado, Advil or Aleve may lessen your discomfort
- You may resume sexual relations two weeks after the procedure, a condom should be used for the first 2 weeks.
- Your semen may be dark brown or black, this is normal and is related bleeding that may have occurred during the implant
- Most men experience burning on urination and/or urinary frequency, continue to take the Flomax as directed
- It is normal to have some blood in your urine for a few days after the implant
Special instructions & info regarding the Iodine seed:
- It is unlikely that you will pass an Iodine-125 seed in your urine, however, as a precaution, please urinate through the strainer for the next week (you would have received this item on discharge)
- The seeds are silver in colour and are the size of a rice grain
- If you do pass a seed, follow the directions in your discharge kit
- Your prostate will absorb the radiation, objects that are touched will not become radioactive
- Body wastes & fluids are not radioactive
- Children & pets should not sit on the patient’s lap for the first 2 weeks after the implant.
Contact your doctor if you experience fever or chills, have increasing pain or unable to urinate


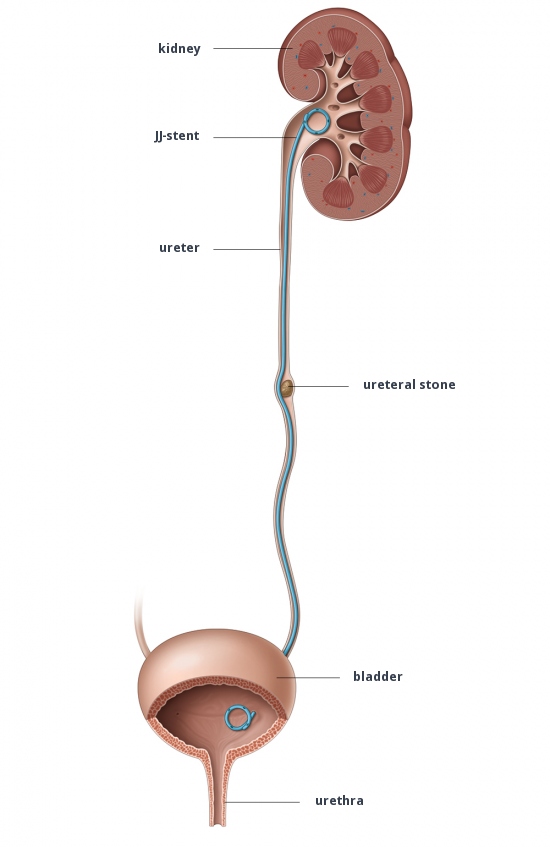 JJ Stent
JJ Stent